Functional Diagnosis (II)
by Pablo V. Romero MD , PhD
Pulmonary function tests explore different aspects of pulmonary (respiratory) function. Usually several categories of parameters can be identified: those exploring ventilation, gas exchange, pulmonary circulation, oxygen transport or response to exercise. Obviously all these parameters interact with one another in such a way that, for instance, ventilatory dysfunction nearly always influences gas exchange or response to exercise, and so on.
Accordingly, the ensemble of parameters (either directly measured or calculated) compose a matrix on which we are able to distinguish “diagnostic vectors” on the basis of parameters pointing in a given direction, but interacting with other parameters that, by themselves would point in another direction. For instance: if an ensemble of parameters point to the existence of bronchial obstruction (low FEV1%FVC, increased RV%TLC, low MEF…) we conclude that bronchial obstruction is the functional diagnosis (diagnostic vector). However, the functional diagnosis can be differently qualified depending on whether there is a DLCO defect or not (that by itself points to a trouble of gas exchange and ventilation/perfusion matching). The same consideration applies to a decrease in PaO2, V’O2max, or TLC, or an increase in PaCO2, Pap, etc. Those interactions qualify our diagnostic vector either in the direction of more or less severity of the disease or by orientating it to a more specific, even different, functional diagnosis. Knowledge of the clinical situation obviously helps in the identification of the main diagnostic vector, but sometimes either we have no clear clinical diagnosis or a given disease may accentuate different functional troubles.
We can therefore consider that the parameters matrix has many interlaced vectors that can draw a functional picture by following a series of steps:
- Indentify main diagnostic vector (ventilatory dysfunction, respiratory insufficiency, pulmonary hypertension…)
- Establish the intensity (mild to very severe)
- Identify the orientation of vector (obstructive, restrictive, mixed…for ventilatory dysfunction)
- Characterize the “color” or main quality (central airways, small airways, diffuse… for obstructive ventilatory disorder)
- Characterize the “shades” (secondary qualities related to this vector: ventilatory heterogeneity, bronchial collapsibility, air trapping…)
- Determine possible interactions between vectors
- Establish the functional diagnosis
The first step consists in identifying the main diagnostic vector. This part is accomplished by looking to parameters that are considered “First Order Parameters”:
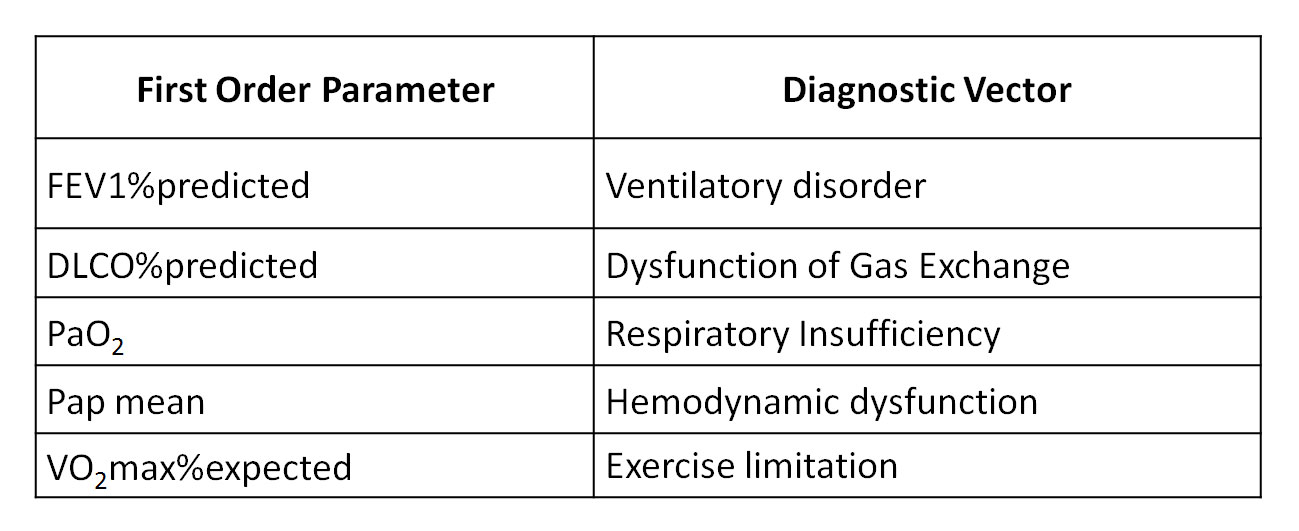
As Lung Function Testing does not usually include hemodynamic studies or exercise tests in an initial evaluation, only Ventilation, Gas Exchange and Oxygen transport disorders can be identified. Exercise limitation and circulatory alterations belong to a second level of functional evaluation and, for the moment, are outside the scope of this article.





